A Comparative Analysis of Sanitation Regulation, Safety Risk, and Government Oversight in Cosmetology Compared with Healthcare, EMS, and Other Public Health Professions.
Research Prepared by
Di Tran University — The College of Humanization
Research & Podcast Series 2026
Research Attribution & Educational Disclaimer
This article is published on Louisville Beauty Academy’s website for educational and informational purposes only.
All research, analysis, and academic interpretation contained in this publication were prepared by Di Tran University — The College of Humanization as part of its independent research initiatives.
Louisville Beauty Academy does not interpret, validate, endorse, or represent the conclusions of this research as regulatory or legal advice. Beauty licensing laws, sanitation regulations, and professional requirements vary by jurisdiction and are determined exclusively by the relevant state licensing authorities, including but not limited to the Kentucky Board of Cosmetology.
Readers should always consult official statutes, administrative regulations, and licensing boards for authoritative guidance.
Publication of this research on the Louisville Beauty Academy website does not constitute policy interpretation, legal guidance, or institutional endorsement.
The Philosophical Foundation of Occupational Stewardship: Professionalism as Humanization
The professional beauty industry, often colloquially associated with the superficial ideals of aesthetics and “pampering,” operates as one of the most rigorously regulated sectors of the United States workforce. At Di Tran University — The College of Humanization, the study of professional licensure is approached not merely as a set of administrative hurdles, but as a fundamental contract between the practitioner and the public’s biological integrity. Occupational licensing in fields such as cosmetology, barbering, esthetics, and nail technology serves as a foundational pillar for public health, safety, and professional standardization.1 These regulations are historically rooted in the transition from medieval guilds to the refined public health mandates of the Progressive Era, a period when the government first recognized that the intimate contact inherent in beauty services could facilitate the transmission of virulent infectious diseases.1
The “hidden safety governance” of the beauty industry is built upon the premise that professional services involve significant biological and chemical risks.1 Practitioners are tasked with managing reactive substances—including hair colors, chemical relaxers, and permanent wave solutions—while simultaneously utilizing sharp, invasive instruments such as razors, shears, and cuticle nippers.1 The intensity of this regulation often surprises the public, particularly when compared to other high-stakes public health professions. For instance, nationally, the average training for a cosmetologist is approximately times longer than the training required for emergency medical technicians (EMTs).2 This disparity, which often provokes political debate, reflects a complex governance strategy: while the EMT is trained for acute, high-intensity life-saving interventions, the cosmetologist is trained for the long-term, high-frequency prevention of community-acquired infections and chronic chemical exposure.2
The legal framework of the industry differentiates between specialty licenses to ensure that practitioners do not inadvertently or intentionally enter the domain of medical practice.1 For example, modern cosmetology statutes emphasize that services must be for “cosmetic purposes” rather than the treatment of physical or mental ailments.1 This boundary is becoming increasingly volatile as the industry moves toward medical-aesthetic integration, where the distinction between a “facial” and a “medical procedure” represents the most contested frontier of medical board jurisdiction.1
The Historical Evolution of Sanitation: From Miasma to Microbes
The current regulatory intensity of the beauty industry is a direct descendant of the “Great Sanitary Awakening” of the mid-nineteenth century. Between and
, public health was dominated by the miasma theory, which posited that diseases like cholera were spread by foul air and environmental filth.3 This led to massive urban engineering projects focused on the literal removal of filth from cities.3 During this era, the skin began to be viewed through a Victorian lens as a “sanitary commissioner” of the body—an organ of drainage that required constant purging of waste materials like sweat and dirt to ensure both health and beauty.4
The revelation of Germ Theory, pioneered by Louis Pasteur and Robert Koch between and
, fundamentally altered this perspective.5 Public health officials shifted their focus from “bad air” to microbial life. This transition mandated greater regulation of all communal spaces, including the barbershop, which was then a known vector for the “barber’s itch”—a highly contagious fungal infection.1 The adoption of Joseph Lister’s principles of antisepsis—originally developed for surgical theaters using carbolic acid in
—eventually became the bedrock of salon sanitation laws.6
Table 1: Historical Milestones in Public Health and Beauty Regulation
| Era | Key Development | Impact on Beauty/Healthcare Regulation | Source |
| Sanitary Movement (UK) | Initial focus on urban cleanliness and filth removal. | 3 | |
| Semmelweis Handwashing | Discovery of hand hygiene as the primary defense against pathogens. | 6 | |
| Lister’s Antisepsis | Introduction of carbolic acid for wound and surface disinfection. | 6 | |
| Germ Theory Adoption | Shift to microbial regulation; birth of modern state health boards. | 5 | |
| Progressive Era | Professional Beauty Acts | Codification of 1,500-hour training to prevent the “Barber’s Itch.” | 1 |
| Founding of the WHO | Establishment of global guidelines for infection prevention. | 6 |
This historical trajectory demonstrates that beauty licensing was never about “beautification” in a vacuum; it was a societal response to the discovery of the invisible microbial world. The high training hours currently required in states like Kentucky ( hours) or Idaho (
hours) are the direct result of this sanitary evolution.8
The Training Hour Paradox: A Comparative Analysis of EMS, Nursing, and Beauty
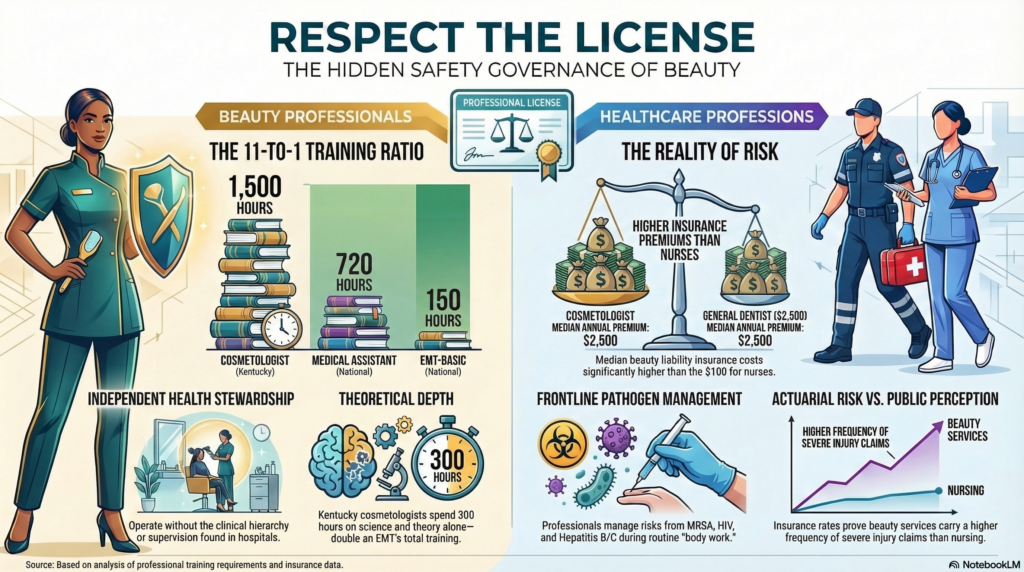
A central point of contention in occupational policy is the “11-to-1” training ratio between cosmetologists and EMTs. This claim, which gained national attention during executive-level discussions on occupational licensing reform, highlights a significant disparity in state-mandated education.2 While the comparison is often used to argue that beauty licensing is over-regulated, a deeper analysis reveals that the educational objectives of these two fields are fundamentally divergent.
The EMT pathway is designed for rapid workforce entry to provide immediate, life-saving stabilization. A national EMT certification requires a state-approved course of at least clock hours.10 In contrast, a cosmetologist in Kentucky must complete
hours of instruction, including
hours dedicated solely to “Science and Theory”—more than double the total training of an EMT.9
Table 2: Comparison of Training Hour Requirements (Selected States/Programs)
| Profession | State/Program | Total Hours | Science/Theory Portion | Source |
| EMT (Basic) | National Standard | Varies by program | 10 | |
| Certified Nursing Assistant (CNA) | Arizona | Varies by program | 10 | |
| Cosmetologist | Kentucky | 9 | ||
| Cosmetologist | Texas | Integrated | 1 | |
| Medical Assistant | National Standard | Integrated | 10 | |
| Esthetician | Kentucky | 9 | ||
| Nail Technician | Texas | Integrated | 12 | |
| Nail Technician | Kentucky | 9 |
The rationale for the high intensity of beauty training lies in the “independent” nature of the work. While a CNA or an EMT operates within a rigid clinical hierarchy—often under the direct or indirect supervision of a physician or nurse—the licensed cosmetologist or barber is frequently the sole individual responsible for the sanitation and chemical safety of their environment.1 The hours of training are intended to build a deep, intuitive understanding of infectious disease prevention, chemical toxicology, and human anatomy to prevent the salon from becoming a focal point for community outbreaks.
In Kentucky, for example, a cosmetology student is legally prohibited from performing chemical services on the public until they have completed at least hours of instruction.9 This “safety buffer” ensures that the student has mastered the theoretical underpinnings of chemical reactions—such as the pH scale of hair relaxers—before they are permitted to handle substances that could cause permanent chemical burns or hair loss.9
Biological Risks and Pathogenic Proliferation in the Modern Salon
The beauty industry is a frontline environment for biological hazard management. Despite the lack of “high-risk” medical procedures, the salon is an ideal incubator for microbes due to the ingredients found in cosmetic products—such as sugar, starch, protein, and fatty acids—and the high water content of many professional formulas.13 Research has identified beauty salons as significant sources of viral, fungal, and bacterial infections.13
Documented biological hazards include common genera such as Staphylococcus, Streptococcus, and Pseudomonas, which are associated with respiratory problems and chronic skin diseases.13 Specific case studies have highlighted the gravity of these risks; for instance, a methicillin-resistant Staphylococcus aureus (MRSA) infection was traced back to a hairdressing visit in London, while unhygienic tools in Nigeria contributed to outbreaks of HIV and Hepatitis.13
Table 3: Microorganisms Isolated from Beauty Salon Tools and Products
| Category | Isolated Microorganisms | Common Source | Source |
| Bacterial | S. aureus, P. aeruginosa, E. coli, Enterobacter spp. | Clippers, brushes, makeup sponges, foot basins. | 13 |
| Fungal | Candida albicans, Aspergillus, Trichophyton, Malassezia | Hairbrushes, nail tools, moist eyeshadows. | 13 |
| Viral | Hepatitis B & C, HIV, Herpes Simplex | Razors, nippers, shared eyeliner/lipstick. | 13 |
| Pathogenic Indicators | P. aeruginosa, S. aureus, Salmonella spp. | Contaminated or expired cosmetic products. | 13 |
In the dental clinic, infection risks are managed with extreme stringency due to the aerosolization of blood and saliva.14 However, the “micro-trauma” caused by a standard manicure or a straight-razor shave provides a sufficient route of transmission for the same bloodborne pathogens. For any pathogen to cause disease, a “chain of infection” must exist: a sufficient number of microorganisms, a reservoir (blood or saliva), a route of transmission, and a susceptible host.15 The 1,500-hour beauty curriculum is designed to systematically break this chain at every stage.
Government Oversight and the Enforcement Architecture
The governance of the beauty industry is maintained through a “Risk-Based” model of inspections, which varies significantly by state. Unlike the healthcare sector, where hospitals and nursing homes face intense, multi-agency oversight (including OSHA, the CDC, and state health departments), beauty establishments are primarily governed by state-specific Boards of Cosmetology or Departments of Licensing.1
In Texas, the Department of Licensing and Regulation (TDLR) classifies violations into three distinct categories based on their threat to public health. This structured enforcement ensures that the “hidden safety governance” is not merely theoretical but is backed by substantial financial penalties.17
Table 4: Texas TDLR Penalty Matrix for Barbering and Cosmetology
| Violation Class | Penalty Range | Example Violation Categories | Source |
| Class A | Administrative errors; failure to display current license; wearing dirty garments. | 17 | |
| Class B | Working with expired license; improper storage of chlorine bleach; failure to clean fixtures. | 17 | |
| Class C | Operating without any license; operating outside the scope of practice; license transfer. | 17 | |
| License Revocation | N/A | Threatening inspectors; repeated Class C violations; major public safety threats. | 17 |
Comparing this to the food service industry reveals a stark difference in regulatory frequency. While high-risk restaurants handling raw meats are often inspected every to
months, many beauty salons are only inspected once per year or even biennially.18 This suggests that the “regulatory intensity” in beauty is front-loaded into the licensure process (the 1,500 hours) rather than the inspection process. The state assumes that if a professional has mastered
hours of training, they are less likely to require constant surveillance than a food handler who may only have completed an 8-hour certification course.21
In California, the Board of Barbering and Cosmetology manages one of the largest regulatory caseloads in the nation. In the fiscal year, the board received
complaints and took
total disciplinary decisions, including
license revocations.23 This enforcement volume highlights the persistent struggle to maintain standards in a fragmented market dominated by small, independent businesses.
Actuarial Insights: The Financial Cost of Professional Negligence
Perhaps the most objective measure of the “hidden risk” in the beauty industry is found in the insurance market. Professional liability insurance, or malpractice insurance, is priced based on the actuarial probability of an incident occurring and the potential cost of that incident.24 Surprisingly, a beautician or cosmetologist often pays significantly more for individual liability coverage than a registered nurse.
While a nurse can obtain an individual malpractice policy for approximately per year, a cosmetologist pays a median cost of
to
per year.25 This
cost ratio indicates that insurance underwriters perceive a higher risk of “frequent and severe” claims in the salon setting compared to the nursing setting.
Table 5: Comparative Professional Liability Insurance Costs (Median Annual)
| Profession | Annual Premium (Median) | Key Risk Factor | Source |
| Registered Nurse (RN) | Medication errors; failure to monitor. | 25 | |
| Dietitian / Nutritionist | Improper dietary advice; allergy issues. | 24 | |
| Cosmetologist / Beautician | Chemical burns; hair loss; eye infections. | 26 | |
| Nurse Practitioner (NP) | Diagnostic errors; prescription authority. | 28 | |
| General Dentist | Nerve damage; surgical complications. | 28 | |
| Oral Surgeon | High-risk surgical procedures. | 28 | |
| General Surgeon | Complex, life-threatening interventions. | 28 |
The claims data in the beauty industry underscores the necessity of high-intensity training. Documented insurance payouts include for hair loss resulting from a treatment and
for chemical conjunctivitis caused by an eyelash extension.30 These are not “superficial” injuries; they represent significant bodily harm and long-term psychological distress. The
hours of training serve as a form of risk mitigation that keeps these premiums from escalating to surgical levels.
The Medical-Aesthetic Integration and the Regulatory Frontier
The integration of aesthetic medicine—minimally invasive procedures like fillers, botulinum toxin, and laser treatments—has created a “gray area” of regulation. In many countries, there is a heated debate between physicians and cosmetologists over who is authorized to perform these procedures.31 Traditional therapeutic medicine centers on disease treatment, while aesthetic medicine centers on the “appreciation of beauty” and the commodification of human worth.31
In the United States, the legal distinction is often tied to the “cosmetic purpose” of the act. A licensed cosmetologist in Kentucky is authorized to provide “facials and massages” but is strictly prohibited from treating “physical or mental ailments”.1 However, as technology advances, the tools used by cosmetologists (such as facial machines and high-intensity lasers) increasingly resemble medical devices.9
The Ministry of Health in various nations, including recent communications from Poland, has attempted to draw a rigid line: procedures like fillers should be performed exclusively by specialist physicians in dermatology or plastic surgery.32 Yet, because many jurisdictions lack a rigid statutory definition of an “aesthetic medicine procedure,” the conflict remains unresolved.32 This regulatory tension highlights the shift of the beauty industry toward a more clinical identity—a transition that Di Tran University identifies as the “humanization of professional aesthetics.”
Sociological Devaluation and the “Pink Tax” of Regulation
Despite the rigorous training and actuarial risk, beauty industry labor is often devalued in sociological discourse. The concept of “aesthetic labor”—the practice of screening and managing workers based on their physical appearance—is often used to stratify workers by class, race, and gender.34 Because the industry is predominantly female, its regulatory mandates are sometimes viewed as “undervalued” or dismissed as unnecessary “economic barriers”.35
Marie Boyd of the University of South Carolina argues that this association with femininity has led to a lack of federal oversight. For example, the FDCA has fewer than two pages devoted to cosmetics out of its 500-page total.35 Unlike drugs, cosmetics do not need FDA approval before they are sold, and manufacturers are not required to report adverse events.35 This places an enormous burden on the individual practitioner; they must be the final “safety filter” for products that the federal government does not adequately monitor.35
Furthermore, the beauty obsession fostered by media and industry messaging has mental health implications, particularly for Generation Z.36 The shift from using cosmetics for “concealment” to “creative expression” reflects a changing consumer psychology that beauty professionals must now manage.36 The 1,500-hour license, therefore, is not just a technical requirement; it is a credential that allows the professional to navigate these complex psychological and physical interactions with authority and ethical responsibility.
Comparative Workplace Safety: Healthcare vs. Beauty Establishments
When examining “Regulatory Intensity,” it is essential to compare the safety outcomes for the workers themselves. Healthcare and social assistance practitioners experience some of the highest rates of workplace injuries in the private sector, with injuries per
full-time workers.38 These injuries are often the result of “safe patient handling” failures or workplace violence.16
In contrast, the risks in beauty establishments are chronic rather than acute. Nail salon workers, predominantly immigrant women, face cumulative exposure to biological, ergonomic, and chemical hazards.41 However, because the beauty industry is dominated by micro-enterprises and independent contractors, many of these “injuries” go unreported to OSHA.41 This lack of centralized data often masks the true “regulatory intensity” needed to protect these workers.
Table 6: Occupational Hazard Comparison: Healthcare vs. Beauty Industry
| Hazard Category | Healthcare Industry Profile | Beauty Industry Profile | Source |
| Infectious Disease | High exposure (Aerosol, Bloodborne) | High exposure (Direct Contact, Skin Flora) | 13 |
| Physical Violence | of all nonfatal workplace violence | Low documented frequency | 39 |
| Chemical Exposure | Disinfectants, Sterilants | Reactive chemicals, Formaldehyde, Monomers | 16 |
| Ergonomic Risk | Patient handling, lifting | Repetitive motion, prolonged standing | 38 |
| Regulatory Lead | OSHA / CDC / State Health | State Boards / TDLR | 16 |
The “hidden safety governance” of the beauty industry acts as a massive public health buffer. By ensuring that trillion microbes on the human skin are managed through proper antisepsis in millions of salons every day, the beauty industry prevents a secondary burden on the healthcare system.7
Conclusions and the Path Forward for Di Tran University
The comprehensive analysis of the beauty industry’s regulatory landscape reveals a profession that is fundamentally misunderstood by the public and often undervalued by policymakers. The hours required for a cosmetology license—
times more than an EMT—is not an accident of history or a product of lobbying; it is a calculated societal response to the biological and chemical risks inherent in “body work.”
At Di Tran University — The College of Humanization, we conclude that the “Respect the License” initiative is a vital component of public health advocacy. The following key insights should guide the future of beauty governance:
- Pedagogical Intensity as Public Health Defense: The high training hours in beauty are essential because the practitioner operates as an independent, frontline steward of sanitation without the institutional “safety net” found in hospitals.
- Actuarial Reality Trumps Political Narrative: The higher cost of professional liability insurance for cosmetologists compared to nurses provides undeniable proof of the “hidden risks” that the license is designed to manage.
- The Biological Burden is Real: With
contamination rates found on unsterilized tools in certain studies, the transition from “Barber’s Itch” to “MRSA” proves that the microbial threat is evolving, not disappearing.
- Regulatory Humanization: Professionalizing the beauty industry through high standards protects the dignity and bodily integrity of the client, fulfilling the core mission of the College of Humanization.
The beauty industry is not a “secondary” health profession; it is a primary prevention sector. As we move into an era of medical-aesthetic integration, the license must be respected as the legal and scientific bedrock that ensures “beauty at any cost” does not become a literal reality for the public’s health.
Works cited
- The Legal Scope of Beauty Licensing in the United States: A …, accessed March 11, 2026, https://louisvillebeautyacademy.net/the-legal-scope-of-beauty-licensing-in-the-united-states-a-comprehensive-policy-legal-and-workforce-analysis-of-cosmetology-barbering-esthetics-and-nail-technology-research-podcast-serie/
- Are cosmetologists training longer than EMTs? | The Fact Checker – YouTube, accessed March 11, 2026, https://m.youtube.com/watch?v=-qm8TipH6fY
- HIST 234 – Lecture 11 – The Sanitary Movement and the “Filth Theory of Disease”, accessed March 11, 2026, https://oyc.yale.edu/history/hist-234/lecture-11
- ‘To Preserve the Skin in Health’: Drainage, Bodily Control and the Visual Definition of Healthy Skin 1835–1900 – PMC, accessed March 11, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC4103382/
- Germ Theory 1880-1912 – Salt Lake County Archives, accessed March 11, 2026, https://www.saltlakecounty.gov/archives/exhibits/the-salt-lake-county-health-department-history/germ-theory/
- History of Hygiene: From Rituals to Modern Standards – CWS, accessed March 11, 2026, https://www.cws.com/en/hygiene/news-knowledge/history-hygiene-invisible-protection-through-ages
- The little-known history of cleanliness and the forgotten pioneers of handwashing – Frontiers, accessed March 11, 2026, https://www.frontiersin.org/journals/public-health/articles/10.3389/fpubh.2022.979464/full
- Training Program Search – IdahoWorks, accessed March 11, 2026, https://idahoworks.gov/search/programs?per_page=10&search_training_program_search%5Baverage_hours_per_week%5D=0&search_training_program_search%5Bhas_certified_curriculum%5D=1&search_training_program_search%5Bprogram_course_time_ids%5D=1
- Title 201 Chapter 12 Regulation 082 • Kentucky Administrative …, accessed March 11, 2026, https://apps.legislature.ky.gov/law/kar/titles/201/012/082/10638/
- Health Services Academy | Applied Technologies Pre-K & 7-12, accessed March 11, 2026, https://www.alaschools.org/az/applied-technologies/academies/health
- Health Science Certificate Training Program in South Florida – Sheridan Technical College, accessed March 11, 2026, https://www.sheridantechnicalcollege.edu/medical-health-science/
- Cosmetology | 2025-2026 Grayson College Catalog, accessed March 11, 2026, https://catalog.grayson.edu/2025-2026/programs/cosmetology/index.php
- Beauty Salons are Key Potential Sources of Disease Spread – PMC, accessed March 11, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC8007475/
- The Unseen Threat in Dentistry: How to Identify, Prevent, and Overcome Infection Risks in the Modern Dental Clinic – jicrcr, accessed March 11, 2026, https://jicrcr.com/index.php/jicrcr/article/download/1789/1512/3733
- Preventing Cross Infection in the Dental Office – StatPearls – NCBI Bookshelf – NIH, accessed March 11, 2026, https://www.ncbi.nlm.nih.gov/books/NBK589669/
- Healthcare – Overview | Occupational Safety and Health Administration, accessed March 11, 2026, https://www.osha.gov/healthcare
- Penalties and Sanctions for Practitioners and Establishments …, accessed March 11, 2026, https://www.tdlr.texas.gov/enforcement/bacsanctions-practitioners-establishments.htm
- Inspection frequency : r/healthinspector – Reddit, accessed March 11, 2026, https://www.reddit.com/r/healthinspector/comments/1lf2ypi/inspection_frequency/
- Understanding Your Food Hygiene Rating: What It Means for Restaurants – KNOW App, accessed March 11, 2026, https://www.getknowapp.com/blog/food-hygiene-rating/
- Inspection Program – MyFloridaLicense.com, accessed March 11, 2026, https://www2.myfloridalicense.com/division-of-regulation/inspection-program/
- Food Safety Training | DuPage County Health, IL, accessed March 11, 2026, https://www.dupagehealth.org/202/Food-Safety-Training
- Health Inspections for Nail Salons and Barbershops – The Institute for Justice, accessed March 11, 2026, https://ij.org/report/clean-cut/health-inspections-for-nail-salons-and-barbershops/
- Enforcement Statistical Overview – California Board of Barbering and Cosmetology – CA.gov, accessed March 11, 2026, https://www.barbercosmo.ca.gov/enforcement/enf_stats.shtml
- Medical Malpractice Insurance Cost: Fast & Free Quotes | Insureon, accessed March 11, 2026, https://www.insureon.com/small-business-insurance/medical-malpractice/cost
- Everything You Need to Know About Nursing Malpractice Insurance, accessed March 11, 2026, https://nurse.org/education/nursing-malpractice-insurance/
- Cosmetology Insurance Cost Guide | Compare side by side – Simply Business, accessed March 11, 2026, https://www.simplybusiness.com/business-insurance/cosmetology-insurance/cost/
- Cosmetologist Insurance | Cosmetology Business Insurance – InsuredBetter.com, accessed March 11, 2026, https://www.insuredbetter.com/small-business-insurance/health-beauty/cosmetologist-coverage/
- How Much Does Medical Malpractice Insurance Cost for Surgeons, Dentists, and Nurses?, accessed March 11, 2026, https://www.finchmccranie.com/blog/how-much-does-medical-malpractice-insurance-cost-for-surgeons-dentists-and-nurses/
- 2024 Medical Professional Liability: An Evolving Landscape, accessed March 11, 2026, https://ppemedical.com/blog/2024-medical-professional-liability-an-evolving-landscape/
- Professional Liability Insurance – Beauty Insurance Plus, accessed March 11, 2026, https://www.beautyinsuranceplus.com/professional-liability-insurance/
- Ethical and Regulatory Gaps in Aesthetic Medical Practice in Top Asian Medical Tourism Destinations – PMC, accessed March 11, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC10776543/
- How Does the Ministry of Health’s Communication Affect the Beauty Industry? | Żyglicka, accessed March 11, 2026, https://www.kpr.pl/en/how-does-the-ministry-of-healths-communication-affect-the-beauty-industry/
- Title 201 Chapter 12 Regulation 082 • Kentucky Administrative Regulations – Legislative Research Commission, accessed March 11, 2026, https://apps.legislature.ky.gov/law/kar/titles/201/012/082/
- Aesthetic Labor for the Sociologies of Work, Gender, and Beauty – ResearchGate, accessed March 11, 2026, https://www.researchgate.net/publication/269280709_Aesthetic_Labor_for_the_Sociologies_of_Work_Gender_and_Beauty
- More Regulation Needed to Combat Risks From Cosmetics | The Regulatory Review, accessed March 11, 2026, https://www.theregreview.org/2019/06/13/fritz-more-regulation-needed-combat-cosmetics-risks/
- Decoding Influence: Cosmetic Industry Strategies, Media Beauty Standards, and Their Mental Health Impact on Generation Z Consume – Digital Collections @ Suffolk, accessed March 11, 2026, https://dc.suffolk.edu/cgi/viewcontent.cgi?article=1045&context=undergrad
- The Beauty Industry’s Influence on Women in Society – UNH Scholars Repository, accessed March 11, 2026, https://scholars.unh.edu/cgi/viewcontent.cgi?article=1085&context=honors
- Top 10 Industries with Highest OSHA Injury Rates (2026) – OSHA Education School, accessed March 11, 2026, https://blog.oshaeducationschool.com/industries-highest-osha-injury-rates/
- OSHA 2025: What Healthcare Professionals Need to Know – Abyde, accessed March 11, 2026, https://abyde.com/2025-osha-healthcare-updates/
- Trends in workplace violence for health care occupations and facilities over the last 10 years, accessed March 11, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC11630250/
- Licensure and citations among nail salons in Michigan from 2017 to 2021: A cross‐sectional study of an overlooked and vulnerable industry – ResearchGate, accessed March 11, 2026, https://www.researchgate.net/publication/362130091_Licensure_and_citations_among_nail_salons_in_Michigan_from_2017_to_2021_A_cross-sectional_study_of_an_overlooked_and_vulnerable_industry
- Employer-Reported Workplace Injuries and Illnesses – 2023-2024 – BLS.gov, accessed March 11, 2026, https://www.bls.gov/news.release/pdf/osh.pdf
- Ten Most Common Code Violations in Establishment Inspections, accessed March 11, 2026, https://www.tdlr.texas.gov/barbering-and-cosmetology/establishments/most-common-violations.htm




